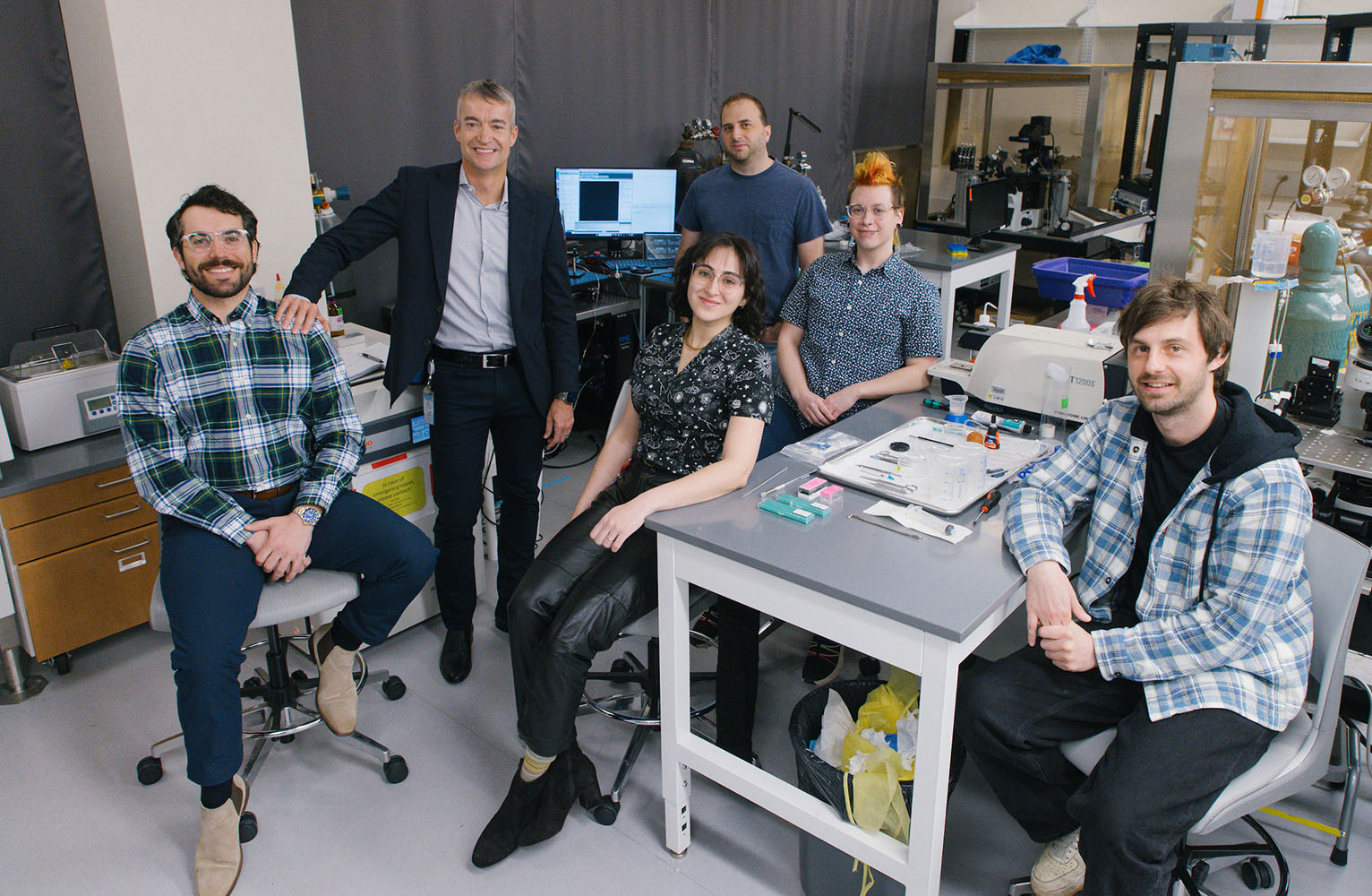
Greg Scherrer (second from left) and his team are developing an entirely new class of therapeutics that relieves pain but is not addictive. (Photo by Jeyhoun Allebaugh)
Novel therapeutic could reduce dual epidemics — chronic pain and opioid use disorder.
One quarter way through the 21st century, the United States finds itself in the grip of two intertwined epidemics: chronic pain and opioid use disorder. An estimated 50 million Americans experience chronic pain, and more than six million have opioid use disorder. In 2023, around 80,000 Americans died from opioid overdose.
UNC School of Medicine Professor Greg Scherrer is tackling both epidemics by developing an entirely new class of therapeutics that relieves pain but is not addictive.
The overdose crisis has sparked worthy attempts at policy changes, logistical improvements and educational efforts to reduce addiction and its consequences. But those are short-term solutions, Scherrer said. “Only novel, transformational non-opioid medicines can provide a long-term and definitive solution to treat chronic pain and end the opioid epidemic.”
To advance this challenging but important research, Scherrer has relied on crucial seed funding from Eshelman Innovation and the NC Collaboratory, which utilizes appropriations received from the North Carolina General Assembly Opioid Abatement Fund.
In the following Q&A, Scherrer explains how he leveraged outside funding and a critical Carolina collaboration to advance his research and land an additional $12 million NIH grant.
Why is pain research so challenging?
There are about 100 billion neurons in the brain. They are important for many different things, including sensations, emotions, thoughts and movement. The challenge is to find those cells that are mostly, if not exclusively, involved in pain perception and try to shut them down.
That’s something opioids do well for many patients — shut down pain perception. But the receptors onto which opioids act are not restricted to pain cells. They are present in neural circuits important for reward. This is why opioids are addictive. Opioid receptors are also present in breathing systems. This is why people can die from overdose, because opioids can shut off respiration.
Among those billion neurons, you want to find the cells that are mostly important for pain and nothing else, and that’s not easy.
Explain your approach.
We’re trying a completely novel approach. For decades, most research has focused on sensory neurons and nerves and how to block pain signals detected in the peripheral organs, the skin, the joints. Instead, we want to target the brain.
People who live with pain complain about the “emotional burden” of being in pain — the unpleasant quality they feel every time they want to do something, and it hurts. Our lab has discovered, in a region of the temporal lobe, a group of brain cells that generate the unpleasant emotional experience of pain. We want to shut them off such that people would still feel the sensation of pain, but it wouldn’t be emotionally draining. They could once again engage in enjoyable activities, like going for a run or playing with the kids or grandkids.
How do you turn that finding into non-addictive painkillers?
Once we found these cells in the brain that make pain unpleasant, we needed to find what proteins to target. My group was kind of stuck. We’re neurobiologists. What we needed was to collaborate with chemists — people who can make small molecules to target these proteins. To advance a novel pain medicine, we collaborated with the lab of Jeffrey Aubé [Eshelman Distinguished Professor in the UNC Eshelman School of Pharmacy] to synthesize numerous candidate compounds, evaluate their pain-relieving properties and select a brain-penetrant compound with favorable properties for further development. The team discovered a compound that significantly reduces both short-term surgical pain and long-lasting nerve pain in preclinical models and reduces behaviors linked to morphine addiction, suggesting it could help treat both pain and opioid use disorder.
Results from this research are reshaping how chronic pain treatments are developed. This work identifies a new, non-opioid class of pain medicines and demonstrates the importance of targeting the brain to treat chronic pain, unlike current approaches that act on peripheral nerves and often fail.
How does funding support this work?
Outside funding has been crucial in many ways. It helped us partner with the Aubé Lab. We’re working together, biologists and chemists, to try to develop novel painkillers. Eshelman Innovation was super helpful in helping us better understand the kind of nitty-gritty science of the drug development process. We leveraged early funding to win a $12 million, multidisciplinary NIH grant. Postdoctoral research David Lee, project manager, plays a critical role in helping us translate our findings into a new class of therapeutics.
Continued support can help us move this strategy from the laboratory to patients, positioning North Carolina institutions as leaders in developing opioid-replacing medicines to treat chronic pain and end the opioid epidemic.
I think we can really change people’s lives. People who suffer from pain, people who are addicted to opioids have very limited options in terms of therapeutics. At UNC, we have all the expertise and strength to develop a novel generation of treatments that will be much more precise.
As told to Logan Ward
Related Stories